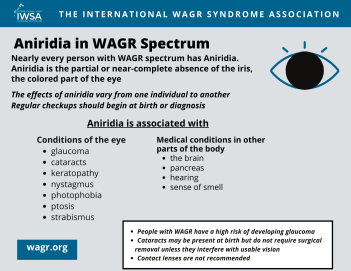
Aniridia is a rare eye condition that involves partial or near-complete absence of the iris, the colored part of the eye. Most people with Aniridia have some iris tissue, though it may be such a small amount that it can only be seen through an ophthalmoscope. Individuals with Aniridia have enlarged pupils, which causes their eyes to appear to be very dark.

Normal Eye
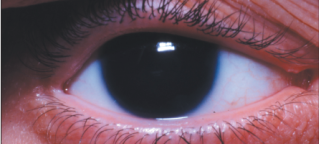
Aniridic Eye
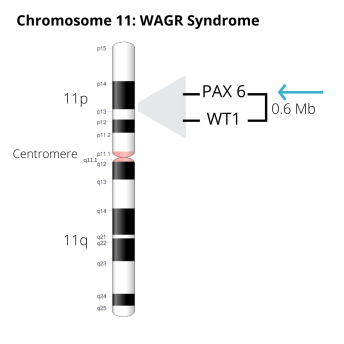
In people with WAGR syndrome, Aniridia occurs as a result of a deletion of one copy of the gene called PAX6. This gene is located on the short (p) arm of Chromosome 11. This type of Aniridia is usually not inherited.
In other cases of Aniridia, both copies of the PAX6 gene are present, but there is a mutation in the gene. When this mutation is inherited from a parent who has Aniridia, it is called Familial Aniridia. Familial Aniridia accounts for about two thirds of all cases.
In about one third of cases, Aniridia is not inherited. This is called Sporadic or Isolated Aniridia.
In very rare cases, Aniridia can be the result of mutations in other genes, including ELP4, FOXC1, PITX2, PITX3, ITPR1, and others.
The impact of Aniridia on vision varies from one individual to another. Many people with Aniridia have functional vision. But Aniridia is associated with numerous other conditions in the eye, including glaucoma, cataracts, Aniridia-associated Keratopathy, and others. Some of these conditions can cause loss of vision, and some may result in blindness.
Aniridia is also associated with medical conditions in other parts of the body. These conditions are thought to be related to the effects of abnormalities in the PAX6 gene, and include problems with the brain, the pancreas, hearing, and sense of smell.
Printable Information Sheet
People with Aniridia have a particularly high risk of developing glaucoma, and it may be challenging to treat. Regular testing for glaucoma should begin at birth.
Cataracts are often present at birth. Cataracts do not require surgical removal unless they interfere with usable vision.
Aniridia-associated Keratopathy (AAK) is also called “corneal pannus.” AAK often begins in childhood or adolescence but may not affect vision until adulthood. Early diagnosis and treatment may help to delay progression.
Other Associated Eye Conditions
Nystagmus in a child with WAGR syndrome
Conditions beyond those in the eye may be present in a person with Aniridia. "Aniridia Syndrome" refers to increasing recognition among researchers and physicians that mutations in the PAX6 gene may affect multiple systems throughout the body. It is important to remember that not all individuals with Aniridia will have or develop all of these conditions.
Many factors influence visual acuity in Aniridia. Visual acuity is the ability to discern shapes and details of the things you see. In Aniridia, the absence of an iris causes a reduction in sharpness of vision, and also causes an increased sensitivity to light (photophobia). Other conditions of the eye that may be present at birth, such as nystagmus or cataracts, or conditions that occur after birth or later in life, such as glaucoma or Aniridia-associated keratopathy, may further reduce vision.
Some individuals with Aniridia are partially sighted or blind, while some have near normal vision. Most people with Aniridia fall somewhere in the middle.
Average visual acuity in Aniridia ranges from about 20/80 to 20/200 (feet) or 6/24 to 6/60 (meters). With a visual acuity of 20/80 (6/24) most people can read large print at about arm's length distance. Visual acuity of 20/200 (6/60) is usually enough to enable a person to see the large "E" on an eyechart, and to read large print at a very close distance.
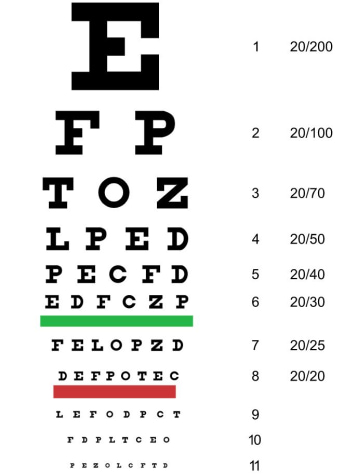
Snellen Eye Chart
Corrective eyeglasses do not improve vision in Aniridia, unless the person also has a "refractive error." Refractive errors included myopia (near-sightedness), hyperopia (far-sightedness), and astigmatism (blurry vision at all distances). Refractive errors are the result of irregularities in the shape of the cornea. These irregularities prevent light from entering the eye at the proper angle for sharp vision. Eyeglasses correct refractive errors by bending the light that enters the eye and refocusing it properly at the back of the eye. If a person with Aniridia has one of these refractive errors, eyeglasses will help to correct it. But eyeglasses cannot correct the other conditions associated with Aniridia that cause diminished vision.
Contact lenses should be used with caution in individuals with Aniridia, as they may hasten the progression of Aniridia-associated Keratopathy (see Associated Conditions).


Light
Indoor lighting is not harmful to people with Aniridia and is generally not bright enough to cause discomfort. Over time, many people with Aniridia find there are some types of indoor lighting that they prefer for reading, schoolwork, and other activities.
Outdoors, bright sunlight may be quite uncomfortable. Even on rainy or overcast days, glare from reflected sunlight may temporarily but significantly reduce vision. Sunglasses can be very helpful, even for very young children with Aniridia.
Low Vision Aids
Many children and adults with Aniridia use devices to help them read, see, and move safely and independently. Examples of these devices include:
In some countries, a child's school may evaluate the need for and provide training in the use of low vision equipment. These services may also be provided through referral by an eye doctor.
Vision
Parents of typically-sighted children usually notice signs of vision in their infants between 2 weeks and 3 months of age. These signs include staring intently at faces, tracking moving faces or brightly colored objects with their eyes, and reaching for objects.
Parents of children with Aniridia often say they did not see these signs in their infants until 4-6 months of age. Though worrisome, delays in development of vision are common in children with Aniridia. Parents can help their baby with Aniridia by providing lots of opportunities for visual stimulation.
Eye Care
Infants with Aniridia should be seen soon after birth by an ophthalmologist (a medical doctor who specializes in care of the eye). Examinations are typically every 6 months in the early years of life but may be more frequent if there are signs of cataracts, glaucoma or other conditions that should be monitored closely. The ophthalmologist may recommend an Exam Under Anesthesia for a young child with Aniridia. These exams usually involve brief, light sedation, and allow for a thorough assessment of the structures of the eye.


The International WAGR Syndrome Association is working to stimulate research on Aniridia.
Educational and Informational Videos from Aniridia North America
Aniridia North America's Focal Point Webinar Series features experts discussing information on a variety of aniridia-related topics. To learn more about Aniridia North America, visit https://aniridiana.org
"Glaucoma in Aniridia - Part 1"
"Glaucoma in Aniridia - Part 2"
"Aniridia 101: How to Care for a Child's Eyes with Aniridia"
Educational and Informational Videos from Aniridia Europe
To learn more about Aniridia Europe, visit https://www.aniridia.
"Managing Aniridia: Dos and Don'ts from Infancy to Adulthood"

Sign up for News & Events
COPYRIGHT© 2025 IWSA / International WAGR Syndrome Association